Journal of Neuro-Oncology ( IF 3.2 ) Pub Date : 2023-02-28 , DOI: 10.1007/s11060-022-04235-w
Kathryn R Tringale 1 , Suzanne L Wolden 1 , Matthias Karajannis 2 , Sofia Haque 3 , Luca Pasquini 3 , Onur Yildirim 3 , Marc Rosenblum 4 , Jamal K Benhamida 4 , Nai-Kong Cheung 2 , Mark Souweidane 5 , Ellen M Basu 2 , Neeta Pandit-Taskar 6 , Pat B Zanzonico 7 , John L Humm 3, 7 , Kim Kramer 2
|
Purpose
Intraventricular compartmental radioimmunotherapy (cRIT) with 131-I-omburtamab is a potential therapy for recurrent primary brain tumors that can seed the thecal space. These patients often previously received external beam radiotherapy (EBRT) to a portion or full craniospinal axis (CSI) as part of upfront therapy. Little is known regarding outcomes after re-irradiation as part of multimodality therapy including cRIT. This study evaluates predictors of response, patterns of failure, and radiologic events after cRIT.
Methods
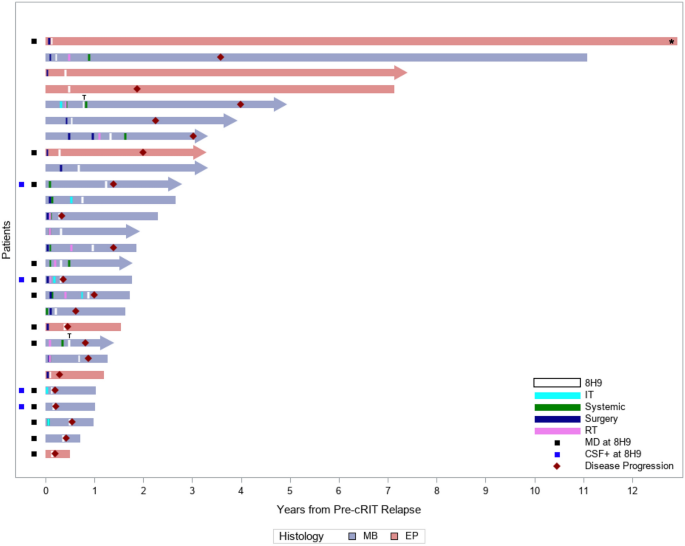
Patients with recurrent medulloblastoma or ependymoma who received 131-I-omburtamab on a prospective clinical trial were included. Extent of disease at cRIT initiation (no evidence of disease [NED] vs measurable disease [MD]) was assessed as associated with progression-free (PFS) and overall survival (OS) by Kaplan–Meier analysis.
Results
All 27 patients (20 medulloblastoma, 7 ependymoma) had EBRT preceding cRIT: most (22, 81%) included CSI (median dose 2340 cGy, boost to 5400 cGy). Twelve (44%) also received EBRT at relapse as bridging to cRIT. There were no cases of radionecrosis. At cRIT initiation, 11 (55%) medulloblastoma and 3 (43%) ependymoma patients were NED, associated with improved PFS (p = 0.002) and OS (p = 0.048) in medulloblastoma. Most relapses were multifocal. With medium follow-up of 3.0 years (95% confidence interval, 1.8–7.4), 6 patients remain alive with NED.
Conclusion
For patients with medulloblastoma, remission at time of cRIT was associated with significantly improved survival outcomes. Relapses are often multifocal, particularly in the setting of measurable disease at cRIT initiation. EBRT is a promising tool to achieve NED status at cRIT initiation, with no cases of radiation necrosis.
中文翻译:
脑室内 131-I-omburtamab 联合外照射放疗治疗复发性髓母细胞瘤和室管膜瘤患者的结局
目的
使用 131-I-omburtamab 的脑室内房室放射免疫治疗 (cRIT) 是一种潜在的治疗方法,用于治疗可植入鞘腔的复发性原发性脑肿瘤。这些患者通常以前接受过部分或全颅脊髓轴 (CSI) 的外照射放疗 (EBRT) 作为前期治疗的一部分。作为包括 cRIT 在内的多模式治疗的一部分,再照射后的结果知之甚少。本研究评估了 cRIT 后反应的预测因子、失败模式和放射学事件。
方法
纳入在前瞻性临床试验中接受 131-I-omburtamab 治疗的复发性髓母细胞瘤或室管膜瘤患者。通过 Kaplan-Meier 分析评估 cRIT 开始时的疾病范围(无疾病证据 [NED] 与可测量疾病 [MD])与无进展 (PFS) 和总生存期 (OS) 相关。
结果
所有 27 例患者 (20 例髓母细胞瘤,7 例室管膜瘤) 在 cRIT 之前都有 EBRT:大多数 (22, 81%) 包括 CSI (中位剂量 2340 cGy,增强至 5400 cGy)。12 例 (44%) 还在复发时接受了 EBRT 作为 cRIT 的桥接。没有放射性坏死病例。在 cRIT 开始时,11 例 (55%) 髓母细胞瘤和 3 例 (43%) 室管膜瘤患者为 NED,与髓母细胞瘤的 PFS (p = 0.002) 和 OS (p = 0.048) 改善相关。大多数复发是多灶性的。在 3.0 年的中期随访 (95% 置信区间,1.8-7.4) 的情况下,6 名患者仍然存活 NED。
结论
对于髓母细胞瘤患者,cRIT 时的缓解与生存结果的显著改善相关。复发通常是多灶性的,尤其是在 cRIT 开始时有可测量疾病的情况下。EBRT 是一种很有前途的工具,可在 cRIT 开始时达到 NED 状态,没有放射性坏死病例。






































 京公网安备 11010802027423号
京公网安备 11010802027423号