Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
重症监护病房 Takotsubo 综合征患者预后列线图的开发和验证:一项回顾性队列研究
Scientific Reports ( IF 3.8 ) Pub Date : 2023-01-10 , DOI: 10.1038/s41598-022-27224-5
Jun Chen 1 , Yimin Wang 1 , Xinyang Shou 1 , Qiang Liu 1 , Ziwei Mei 2
Affiliation
|
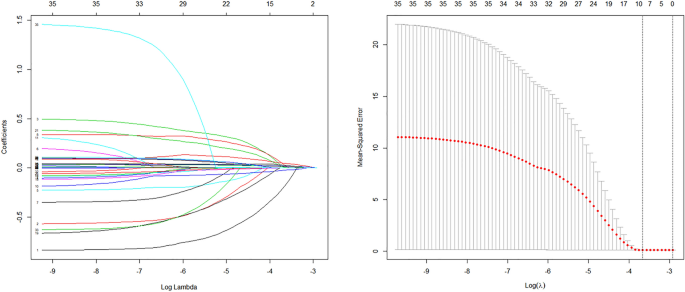
入住重症监护病房 (ICU) 的 Takotsubo 综合征 (TTS) 患者总是比心脏病科住院的患者面临更高的院内死亡风险。后者的预后经过大量研究分析。然而,尚无实用模型来预测 ICU 中 TTS 患者的院内死亡风险。本研究旨在建立一个预测入住 ICU 的 TTS 患者院内死亡的模型。我们回顾性地纳入 MIMIC-IV 数据库中患有 TTS 的 ICU 患者。列线图的结果是院内死亡。最小绝对收缩选择算子(LASSO)分析初步选择了预测变量。该模型是通过多变量逻辑回归分析开发的。校准、决策曲线分析 (DCA) 和受试者工作特征 (ROC) 分别测量列线图在准确性、临床实用性和辨别力方面的性能。最终,368 名 ICU 患有 TTS 的患者参与了这项研究。院内死亡率为13.04%。 LASSO 回归和多变量逻辑回归分析验证了与院内死亡率显着相关的危险因素。它们是钾、凝血酶原时间(PT)、年龄、心肌梗塞、白细胞计数(WBC)、血细胞比容、阴离子间隙和序贯器官衰竭评估(SOFA)评分。该列线图很好地区分了有院内死亡风险的患者。训练集中的曲线下面积 (AUC) 为 0.779 (95%CI: 0.732–0.826),测试集中的曲线下面积 (AUC) 为 0.775 (95%CI: 0.711–0.839)。校准图和 DCA 显示该列线图具有良好的临床效益。我们开发了列线图来预测 ICU 患有 TTS 患者的院内死亡概率。 该列线图能够区分院内死亡风险高的患者并具有临床实用性。
"点击查看英文标题和摘要"






























 京公网安备 11010802027423号
京公网安备 11010802027423号