背景
X连锁低磷血症性佝偻病(XLH)的严重程度可能受基因型和性别的影响。然而,burosumab 是一种针对成纤维细胞生长因子 23 的全人源化单克隆抗体,对男女儿童的推荐剂量相同(每两周 0.8 毫克/公斤)。
患者和方法
在一项回顾性队列研究中,我们描述了 XLH 儿童中不同性别的 burosumab 反应差异。
结果
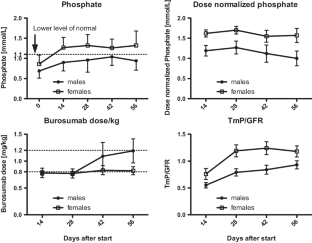
我们使用 XLH 联合 burosumab 治疗了 10 名儿童(5 名女性,起始平均年龄 4.2 ± 3.5 岁)。男性初始平均血清磷酸盐为 0.69 ± 0.18 mmol/L,女性为 0.86 ± 0.22 mmol/L ( p = 0.108)。肾小管磷酸盐最大重吸收率与肾小球滤过率 (TmP/GFR) 的平均比值,男性为 0.55 ± 0.11 mmol/L,女性为 0.76 ± 0.23 mmol/L (p = 0.06 ) 。burosumab 的平均起始剂量为每 14 天皮下注射 0.83 ± 0.19 mg/kg(男性:0.79 ± 0.19 mg/kg;女性:0.87 ± 0.21 mg/kg,ns)。开始 burosumab 两周后,男性 (0.90 ± 0.21 mmol/L) 和女性 (1.27 ± 0.25 mmol/L) 之间的血清磷酸盐存在显着差异 ( p = 0.018)。所有男性都需要增加剂量才能使血清磷酸盐正常化。开始后第 140 天,雄性的平均剂量进一步增加至 1.24 ± 0.41 mg/kg,以达到 0.87 ± 0.11 mmol/L 的磷酸盐,而雌性在起始剂量上具有正常的磷酸盐和碱性磷酸酶。平均 458 ± 79 天后,男性平均 burosumab 剂量/kg 为 1.68 ± 0.61 mg/kg,平均血清磷酸盐为 1.08 ± 0.23 mmol/L,平均 TmP/GFR 为 1.01 ± 0.20,平均碱性磷酸酶已正常化至 303.6 ± 40.7U/L,平均 1.25(OH) 2维生素 D 水平为 186.4 ± 16.6 nmol/L。
结论
我们的研究结果可能表明 XLH 患者对 burosumab 的反应存在性别差异。我们的数据表明男性可能需要更高的剂量。
 "点击查看英文标题和摘要"
"点击查看英文标题和摘要"
Sex differences of burosumab in children with X-linked hypophosphataemic rickets
Background
The severity of X-linked hypophosphataemic rickets (XLH) may be affected by genotype and sex. However, burosumab, a fully humanized monoclonal antibody against fibroblast growth factor 23, has the same pediatric dose recommendation for both sexes (0.8 mg/kg every 2 weeks).
Patients and methods
In a retrospective cohort study, we describe the burosumab response differences by sex in children with XLH.
Results
We treated 10 children (5 females, mean age at initiation 4.2 ± 3.5 years) with XLH with burosumab. Initial mean serum phosphate was 0.69 ± 0.18 mmol/L in males and 0.86 ± 0.22 mmol/L in females (p = 0.108). The mean ratio of tubular maximum reabsorption rate of phosphate to glomerular filtration rate (TmP/GFR) was 0.55 ± 0.11 mmol/L in males and 0.76 ± 0.23 mmol/L in females (p = 0.06). The mean starting dose of burosumab was 0.83 ± 0.19 mg/kg subcutaneously every 14 days (males: 0.79 ± 0.19 mg/kg; females: 0.87 ± 0.21 mg/kg, n.s.). Two weeks after starting burosumab, serum phosphate differed significantly between males (0.90 ± 0.21 mmol/L) and females (1.27 ± 0.25 mmol/L) (p = 0.018). All males required a dose increase to try to normalize serum phosphate. On day 140 after starting, the average dose in males increased further to 1.24 ± 0.41 mg/kg to achieve a phosphate of 0.87 ± 0.11 mmol/L while females had a normal phosphate and alkaline phosphatase on the starting dose. After a mean of 458 ± 79 days, the mean burosumab dose/kg in males was 1.68 ± 0.61 mg/kg, mean serum phosphate was 1.08 ± 0.23 mmol/L, mean TmP/GFR was 1.01 ± 0.20, mean alkaline phosphatase had normalized to 303.6 ± 40.7U/L, and mean 1.25(OH)2 vitamin D level was 186.4 ± 16.6 nmol/L.
Conclusions
Our findings may suggest a sex difference in response to burosumab in XLH patients. Our data suggest that males may require higher doses.



















































 京公网安备 11010802027423号
京公网安备 11010802027423号