Neuroradiology ( IF 2.4 ) Pub Date : 2022-11-22 , DOI: 10.1007/s00234-022-03092-8 Marcel Opitz 1 , Celina Zenk 1 , Sebastian Zensen 1 , Denise Bos 1 , Yan Li 1 , Hanna Styczen 1 , Marvin Darkwah Oppong 2 , Ramazan Jabbarli 2 , Tim Hagenacker 3 , Michael Forsting 1 , Isabel Wanke 1, 4 , Cornelius Deuschl 1
|
Purpose
Endovascular treatment of unruptured intracranial aneurysms (UIAs) requires a risk–benefit analysis and adherence to diagnostic reference levels (DRLs). The national DRL (250 Gy·cm2) is only determined for intracranial aneurysm coiling in general, including ruptured intracranial aneurysms (RIAs). This study aims to investigate the dose in the treatment of UIAs and RIAs separately.
Methods
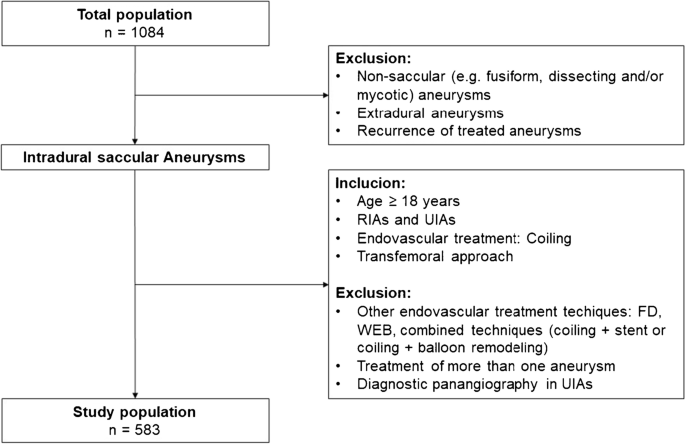
In a retrospective study design, dose area product (DAP) and fluoroscopy time (FT) were assessed for all patients undergoing intracranial aneurysm coiling between 2010 and 2021. DRL was set as the 75th percentile of the dose distribution. A multivariable linear regression analysis was performed to investigate DAP and FT for the two groups, UIA and RIA adjusted for patient age, aneurysm size, and location.
Results
583 (414 females, mean age 56.5 years, 311 UIAs) are included. In the overall population, DAP (median (IQR)) is 157 Gy·cm2 (108–217) with a median FT of 32.7 min (IQR 24.0–47.0). Local DRL is 183 Gy·cm2 for UIAs and 246 Gy·cm2 for RIAs. After adjustment for the other variables, the UIA and RIA groups have a significant effect on both DAP (p < 0.001; 95% CI − 68.432 – − 38.040) and FT (p < 0.001; 95% CI − 628.279 – − 291.254). In general, both DAP and FT increase significantly with patient age and aneurysm size, whereas the location of the aneurysm did not significantly change neither DAP (p = 0.171; 95% CI − 5.537–31.065) nor FT (p = 0.136; 95% CI − 357.391–48.508).
Conclusion
Both aneurysm size and patient age were associated with increased DAP, whereas aneurysm location did not significantly change DAP or FT. The increased dose in patients with RIAs is likely equivalent to additional diagnostic cerebral four-vessel angiography performed in this group.
中文翻译:
未破裂和破裂颅内动脉瘤患者动脉瘤弹簧圈的辐射剂量和透视时间与动脉瘤大小、位置和患者年龄的关系
目的
未破裂颅内动脉瘤 (UIA) 的血管内治疗需要进行风险效益分析并遵守诊断参考水平 (DRL)。国家DRL(250 Gy·cm 2 )仅适用于一般颅内动脉瘤弹簧圈栓塞,包括破裂的颅内动脉瘤(RIA)。本研究旨在分别研究 UIAs 和 RIA 治疗中的剂量。
方法
在一项回顾性研究设计中,对 2010 年至 2021 年间所有接受颅内动脉瘤弹簧圈栓塞术的患者的剂量面积乘积 (DAP) 和透视时间 (FT) 进行了评估。DRL 被设置为剂量分布的第 75 个百分位。进行多变量线性回归分析以研究两组的 DAP 和 FT,UIA 和 RIA 根据患者年龄、动脉瘤大小和位置进行调整。
结果
其中包括 583 名(414 名女性,平均年龄 56.5 岁,311 名 UIA)。在总体人群中,DAP(中位 (IQR))为 157 Gy·cm 2 (108–217),中位 FT 为 32.7 分钟 (IQR 24.0–47.0)。 UIAs 的局部 DRL 为 183 Gy·cm 2 ,RIA 的局部 DRL 为 246 Gy·cm 2 。调整其他变量后,UIA 和 RIA 组对 DAP ( p < 0.001; 95% CI − 68.432 – − 38.040) 和 FT ( p < 0.001; 95% CI − 628.279 – − 291.254) 均具有显着影响)。一般来说,DAP 和 FT 均随着患者年龄和动脉瘤大小而显着增加,而动脉瘤的位置则没有显着改变 DAP ( p = 0.171; 95% CI − 5.537–31.065) 和 FT ( p = 0.136; 95%) CI - 357.391–48.508)。
结论
动脉瘤大小和患者年龄均与 DAP 增加相关,而动脉瘤位置并未显着改变 DAP 或 FT。 RIA 患者增加的剂量可能相当于在该组中进行额外的诊断性脑四血管血管造影。





























 京公网安备 11010802027423号
京公网安备 11010802027423号