Neurocritical Care ( IF 3.1 ) Pub Date : 2022-09-15 , DOI: 10.1007/s12028-022-01586-0 Louis A Gomez 1 , Qi Shen 2 , Kevin Doyle 2 , Athina Vrosgou 2 , Angela Velazquez 2 , Murad Megjhani 2 , Shivani Ghoshal 2, 3 , David Roh 2, 3 , Sachin Agarwal 2, 3 , Soojin Park 2, 3 , Jan Claassen 2, 3 , Samantha Kleinberg 1
|
Background
Impaired consciousness is common in intensive care unit (ICU) patients, and an individual’s degree of consciousness is crucial to determining their care and prognosis. However, there are no methods that continuously monitor consciousness and alert clinicians to changes. We investigated the use of physiological signals collected in the ICU to classify levels of consciousness in critically ill patients.
Methods
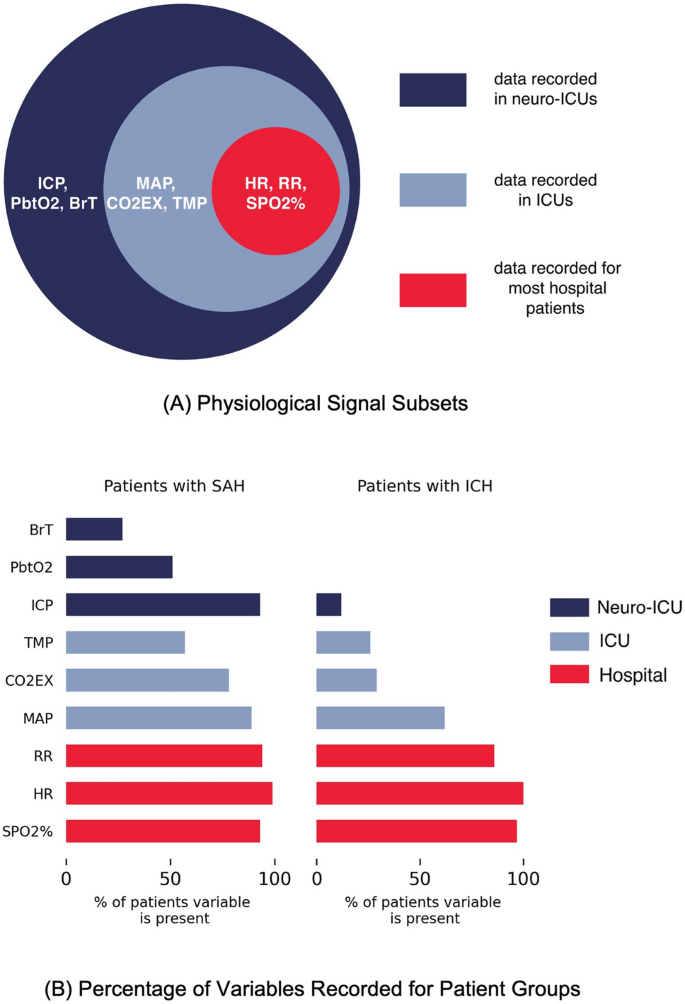
We studied 61 patients with subarachnoid hemorrhage (SAH) and 178 patients with intracerebral hemorrhage (ICH) from the neurological ICU at Columbia University Medical Center in a retrospective observational study of prospectively collected data. The level of consciousness was determined on the basis of neurological examination and mapped to comatose, vegetative state or unresponsive wakefulness syndrome (VS/UWS), minimally conscious minus state (MCS−), and command following. For each physiological signal, we extracted time-series features and performed classification using extreme gradient boosting on multiple clinically relevant tasks across subsets of physiological signals. We applied this approach independently on both SAH and ICH patient groups for three sets of variables: (1) a minimal set common to most hospital patients (e.g., heart rate), (2) variables available in most ICUs (e.g., body temperature), and (3) an extended set recorded mainly in neurological ICUs (absent for the ICH patient group; e.g., brain temperature).
Results
On the commonly performed classification task of VS/UWS versus MCS−, we achieved an area under the receiver operating characteristic curve (AUROC) in the SAH patient group of 0.72 (sensitivity 82%, specificity 57%; 95% confidence interval [CI] 0.63–0.81) using the extended set, 0.69 (sensitivity 83%, specificity 51%; 95% CI 0.59–0.78) on the variable set available in most ICUs, and 0.69 (sensitivity 56%, specificity 78%; 95% CI 0.60–0.78) on the minimal set. In the ICH patient group, AUROC was 0.64 (sensitivity 56%, specificity 65%; 95% CI 0.55–0.74) using the minimal set and 0.61 (sensitivity 50%, specificity 80%; 95% CI 0.51–0.71) using the variables available in most ICUs.
Conclusions
We find that physiological signals can be used to classify states of consciousness for patients in the ICU. Building on this with intraday assessments and increasing sensitivity and specificity may enable alarm systems that alert physicians to changes in consciousness and frequent monitoring of consciousness throughout the day, both of which may improve patient care and outcomes.
中文翻译:
使用生理数据对神经 ICU 中的意识水平进行分类
背景
意识障碍在重症监护病房 (ICU) 患者中很常见,个人的意识程度对于决定他们的护理和预后至关重要。然而,没有任何方法可以持续监测意识并提醒临床医生注意变化。我们调查了使用在 ICU 中收集的生理信号来对危重病人的意识水平进行分类。
方法
我们在一项前瞻性收集数据的回顾性观察研究中,对来自哥伦比亚大学医学中心神经 ICU 的 61 名蛛网膜下腔出血 (SAH) 患者和 178 名脑出血 (ICH) 患者进行了研究。意识水平是在神经系统检查的基础上确定的,并映射到昏迷、植物人状态或反应迟钝的觉醒综合症 (VS/UWS)、最低意识负状态 (MCS−) 和命令遵循。对于每个生理信号,我们提取时间序列特征,并使用极端梯度增强对生理信号子集上的多个临床相关任务进行分类。我们将这种方法独立应用于 SAH 和 ICH 患者组的三组变量:(1) 大多数医院患者共有的最小集合(例如,心率),
结果
在 VS/UWS 与 MCS 的常用分类任务中,我们在 SAH 患者组中实现了接受者操作特征曲线下面积 (AUROC) 0.72(灵敏度 82%,特异性 57%;95% 置信区间 [CI] 0.63–0.81) 使用扩展集,0.69(敏感性 83%,特异性 51%;95% CI 0.59–0.78)在大多数 ICU 可用的变量集上,0.69(敏感性 56%,特异性 78%;95% CI 0.60 –0.78) 在最小集上。在 ICH 患者组中,使用最小集的 AUROC 为 0.64(敏感性 56%,特异性 65%;95% CI 0.55-0.74),使用变量的 AUROC 为 0.61(敏感性 50%,特异性 80%;95% CI 0.51-0.71)在大多数 ICU 中可用。
结论
我们发现生理信号可用于对 ICU 患者的意识状态进行分类。在此基础上,通过日内评估和提高敏感性和特异性,可以启用警报系统,提醒医生意识的变化和全天频繁监测意识,这两者都可以改善患者护理和结果。














































 京公网安备 11010802027423号
京公网安备 11010802027423号