Nature Medicine ( IF 58.7 ) Pub Date : 2022-08-25 , DOI: 10.1038/s41591-022-01977-y
Miranda Gogishvili 1 , Tamar Melkadze 2 , Tamta Makharadze 3 , Davit Giorgadze 4 , Mikhail Dvorkin 5 , Konstantin Penkov 6 , Konstantin Laktionov 7 , Gia Nemsadze 8 , Marina Nechaeva 9 , Irina Rozhkova 10 , Ewa Kalinka 11 , Christian Gessner 12, 13 , Brizio Moreno-Jaime 14 , Rodolfo Passalacqua 15 , Siyu Li 16 , Kristina McGuire 16 , Manika Kaul 16 , Anne Paccaly 16 , Ruben G W Quek 16 , Bo Gao 16 , Frank Seebach 16 , David M Weinreich 16 , George D Yancopoulos 16 , Israel Lowy 16 , Giuseppe Gullo 16 , Petra Rietschel 16
|
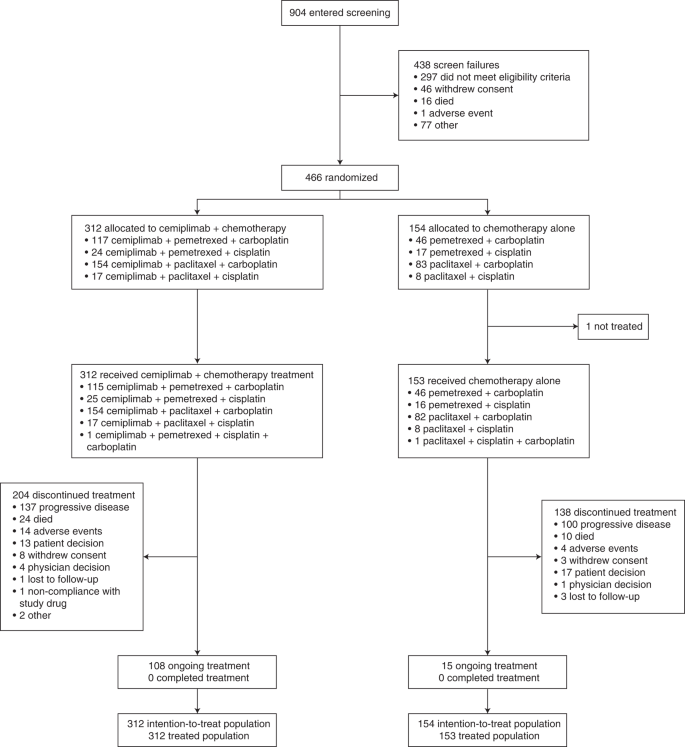
First-line cemiplimab (anti-programmed cell death-1 (PD-1)) monotherapy has previously shown significant improvement in overall survival (OS) and progression-free survival (PFS) versus chemotherapy in patients with advanced non-small cell lung cancer (aNSCLC) and PD-ligand 1 (PD-L1) expression ≥50%. EMPOWER-Lung 3 (NCT03409614), a double-blind, placebo-controlled, phase 3 study, examined cemiplimab plus platinum-doublet chemotherapy as first-line treatment for aNSCLC, irrespective of PD-L1 expression or histology. In this study, 466 patients with stage III/IV aNSCLC without EGFR, ALK or ROS1 genomic tumor aberrations were randomized (2:1) to receive cemiplimab 350 mg (n = 312) or placebo (n = 154) every 3 weeks for up to 108 weeks in combination with four cycles of platinum-doublet chemotherapy (followed by pemetrexed maintenance as indicated). In total, 57.1% (266/466 patients) had non-squamous NSCLC, and 85.2% (397/466 patients) had stage IV disease. The primary endpoint was OS. The trial was stopped early per recommendation of the independent data monitoring committee, based on meeting preset OS efficacy criteria: median OS was 21.9 months (95% confidence interval (CI), 15.5–not evaluable) with cemiplimab plus chemotherapy versus 13.0 months (95% CI, 11.9–16.1) with placebo plus chemotherapy (hazard ratio (HR) = 0.71; 95% CI, 0.53–0.93; P = 0.014). Grade ≥3 adverse events occurred with cemiplimab plus chemotherapy (43.6%, 136/312 patients) and placebo plus chemotherapy (31.4%, 48/153 patients). Cemiplimab is only the second anti-PD-1/PD-L1 agent to show efficacy in aNSCLC as both monotherapy and in combination with chemotherapy for both squamous and non-squamous histologies.
中文翻译:
Cemiplimab 联合化疗与单独化疗治疗非小细胞肺癌:一项随机、对照、双盲 3 期试验
一线 cemiplimab(抗程序性细胞死亡-1 (PD-1))单药疗法先前显示,与化疗相比,晚期非小细胞肺癌患者的总生存期 (OS) 和无进展生存期 (PFS) 有显着改善(aNSCLC) 和 PD-配体 1 (PD-L1) 表达≥50%。EMPOWER-Lung 3 (NCT03409614) 是一项双盲、安慰剂对照的 3 期研究,检查了 cemiplimab 联合铂类双药化疗作为 aNSCLC 的一线治疗,无论 PD-L1 表达或组织学如何。在这项研究中,466 名无EGFR、ALK或ROS1基因组肿瘤畸变的 III/IV 期 aNSCLC 患者被随机 (2:1) 接受 cemiplimab 350 mg ( n = 312) 或安慰剂 ( n = 154) 每 3 周一次,最多 108 周,联合四个周期的铂类双药化疗(随后按指示进行培美曲塞维持治疗)。总共有 57.1%(266/466 名患者)患有非鳞状 NSCLC,85.2%(397/466 名患者)患有 IV 期疾病。主要终点是 OS。根据独立数据监测委员会的建议,该试验根据预设的 OS 疗效标准提前停止:cemiplimab 联合化疗的中位 OS 为 21.9 个月(95% 置信区间 (CI),15.5-不可评估)对比 13.0 个月(95 % CI, 11.9–16.1) 与安慰剂联合化疗(风险比 (HR) = 0.71;95% CI, 0.53–0.93;P = 0.014)。cemiplimab 联合化疗(43.6%,136/312 名患者)和安慰剂联合化疗(31.4%,48/153 名患者)发生了 ≥ 3 级不良事件。Cemiplimab 是第二种在 aNSCLC 中显示疗效的抗 PD-1/PD-L1 药物,既可以作为单一疗法,也可以与化疗联合用于鳞状和非鳞状组织学。






























 京公网安备 11010802027423号
京公网安备 11010802027423号