Leukemia ( IF 12.8 ) Pub Date : 2022-08-16 , DOI: 10.1038/s41375-022-01667-1 Heiner Zimmermann 1, 2 , Christian Koenecke 3 , Martin H Dreyling 4 , Christiane Pott 5 , Ulrich Dührsen 6 , Dennis Hahn 7 , Norbert Meidenbauer 8 , Ingeborg A Hauser 9 , Mathias J Rummel 10 , Dominik Wolf 11, 12 , Michael Heuser 3 , Christian Schmidt 4 , Peter Schlattmann 13 , Matthias Ritgen 5 , Reiner Siebert 14 , Ilske Oschlies 15 , Ioannis Anagnostopoulos 16 , Ralf U Trappe 1, 5
|
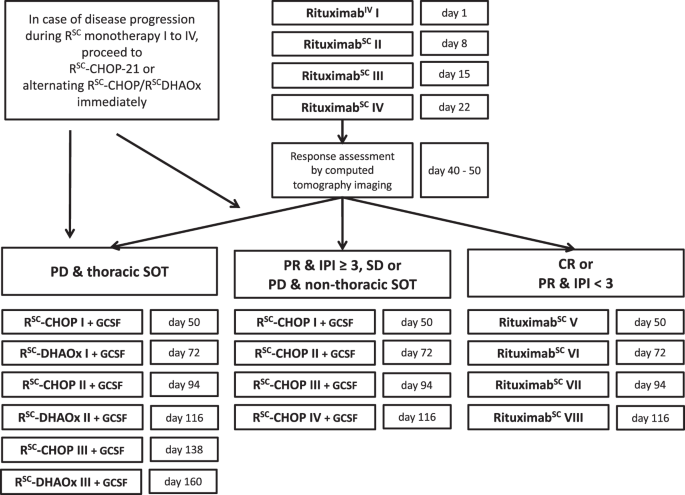
The prospective multicentre Phase II PTLD-2 trial (NCT02042391) tested modified risk-stratification in adult SOT recipients with CD20-positive PTLD based on principles established in the PTLD-1 trials: sequential treatment and risk-stratification. After rituximab monotherapy induction, patients in complete remission as well as those in partial remission with IPI < 3 at diagnosis (low-risk) continued with rituximab monotherapy and thus chemotherapy free. Most others (high-risk) received R-CHOP-21. Thoracic SOT recipients who progressed (very-high-risk) received alternating R-CHOP-21 and modified R-DHAOx. The primary endpoint was event-free survival (EFS) in the low-risk group. The PTLD-1 trials provided historical controls. Rituximab was applied subcutaneously. Of 60 patients enrolled, 21 were low-risk, 28 high-risk and 9 very-high-risk. Overall response was 45/48 (94%, 95% CI 83–98). 2-year Kaplan–Meier estimates of time to progression and overall survival were 78% (95% CI 65–90) and 68% (95% CI 55–80) – similar to the PTLD-1 trials. Treatment-related mortality was 4/59 (7%, 95% CI 2–17). In the low-risk group, 2-year EFS was 66% (95% CI 45–86) versus 52% in the historical comparator that received CHOP (p = 0.432). 2-year OS in the low-risk group was 100%. Results with R-CHOP-21 in high-risk patients confirmed previous results. Immunochemotherapy intensification in very-high-risk patients was disappointing.
中文翻译:
实体器官移植 (SOT) 后 B 细胞移植后淋巴组织增生性疾病 (PTLD) 的改良风险分层序贯治疗(皮下利妥昔单抗联合或不联合化疗):前瞻性多中心 II 期 PTLD-2 试验
前瞻性多中心 II 期 PTLD-2 试验 (NCT02042391) 根据 PTLD-1 试验中确立的原则测试了 CD20 阳性 PTLD 成人 SOT 接受者的改良风险分层:序贯治疗和风险分层。在利妥昔单抗单药诱导后,完全缓解的患者以及诊断时 IPI < 3 的部分缓解患者(低风险)继续接受利妥昔单抗单药治疗,因此无需化疗。大多数其他人(高风险)接受了 R-CHOP-21。进展(非常高风险)的胸部 SOT 接受者交替接受 R-CHOP-21 和改良的 R-DHAOx。主要终点是低风险组的无事件生存期(EFS)。PTLD-1 试验提供了历史对照。皮下应用利妥昔单抗。在入组的 60 名患者中,21 名低风险、28 名高风险和 9 名非常高风险。总体反应为 45/48 (94%, 95% CI 83–98)。2 年 Kaplan-Meier 估计的进展时间和总生存期分别为 78%(95% CI 65-90)和 68%(95% CI 55-80)——与 PTLD-1 试验相似。治疗相关死亡率为 4/59(7%,95% CI 2-17)。在低风险组中,2 年 EFS 为 66%(95% CI 45-86),而在接受 CHOP 的历史对照组中为 52%(p = 0.432)。低风险组的 2 年 OS 为 100%。R-CHOP-21 在高危患者中的结果证实了之前的结果。高危患者的免疫化疗强化令人失望。
































 京公网安备 11010802027423号
京公网安备 11010802027423号