Updates in Surgery ( IF 2.4 ) Pub Date : 2022-07-01 , DOI: 10.1007/s13304-022-01317-2 Matteo Palmeri 1 , Andrea Peri 2 , Valentina Pucci 1 , Niccolò Furbetta 1 , Virginia Gallo 2 , Gregorio Di Franco 1 , Anna Pagani 3 , Chiara Dauccia 3 , Camilla Farè 2 , Desirée Gianardi 1 , Simone Guadagni 1 , Matteo Bianchini 1 , Annalisa Comandatore 1 , Gianluca Masi 4 , Chiara Cremolini 4 , Beatrice Borelli 4 , Luca Emanuele Pollina 5 , Giulio Di Candio 1 , Andrea Pietrabissa 2 , Luca Morelli 1, 6
|
Background
Conventional Right Colectomy with D2 lymphadenectomy (RC-D2) currently represent the most common surgical treatment of right-sided colon cancer (RCC). However, whether it should be still considered a standard of care, or replaced by a routine more extended D3 lymphadenectomy remains unclear. In the present study, we aim to critically review the patterns of relapse and the survival outcomes obtained from our 11-year experience of RC-D2.
Methods
Clinical data of 489 patients who underwent RC-D2 for RCC at two centres, from January 2009 to January 2020, were retrospectively reviewed. Patients with synchronous distant metastases and/or widespread nodal involvement at diagnosis were excluded. Post-operative clinical–pathological characteristics and survival outcomes were evaluated including the pattern of disease relapse.
Results
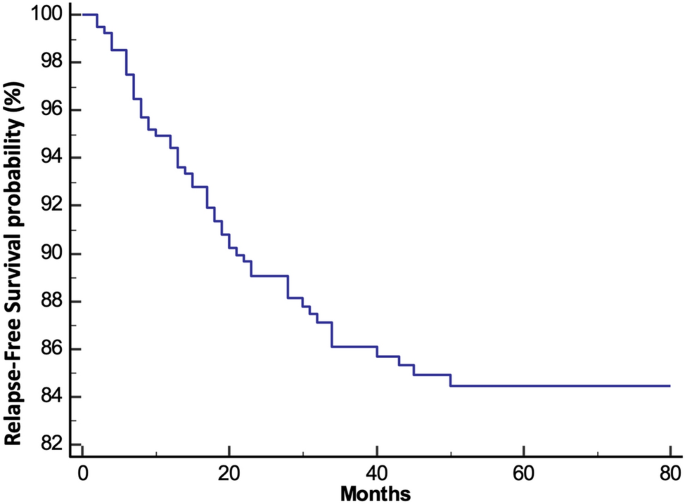
We enrolled a total of 400 patients with information follow-up. Postoperative morbidity was 14%. The median follow-up was 62 months. Cancer recurrence was observed in 55 patients (13.8%). Among them, 40 patients (72.7%) developed systemic metastases, and lymph-node involvement was found in 7 cases (12.8%). None developed isolated central lymph-node metastasis (CLM), in the D3 site. The estimated 3- and 5-year relapse-free survival were 86.1% and 84.4%, respectively. The estimated 3- and 5-year cancer-specific OS were 94.5% and 92.2%, respectively.
Conclusions
The absence of isolated CLM, as well as the cancer-specific OS reported in our series, support the routine use of RC-D2 for RCC. However, D3 lymphadenectomy may be recommended in selected patients, such as those with pre-operatively known CLM, or with lymph-node metastases close to the origin of the ileocolic vessels.
中文翻译:
癌症 D2 右结肠切除术后的复发和生存模式:是否有地方进行常规的更广泛的淋巴结清扫术?
背景
常规右侧结肠切除术联合 D2 淋巴结切除术 (RC-D2) 目前是右侧结肠癌 (RCC) 最常见的手术治疗方法。然而,它是否仍应被视为标准治疗,或被常规更广泛的 D3 淋巴结清扫术所取代,仍不清楚。在本研究中,我们旨在批判性地审查复发模式和从我们 11 年的 RC-D2 经验中获得的生存结果。
方法
回顾性分析了 2009 年 1 月至 2020 年 1 月在两个中心接受 RC-D2 治疗 RCC 的 489 名患者的临床数据。诊断时有同步远处转移和/或广泛淋巴结受累的患者被排除在外。评估术后临床病理特征和生存结果,包括疾病复发的模式。
结果
我们共招募了 400 名患者,并进行了信息随访。术后并发症发生率为 14%。中位随访时间为 62 个月。55 名患者 (13.8%) 出现癌症复发。其中40例(72.7%)发生全身转移,7例(12.8%)淋巴结受累。没有人在 D3 部位出现孤立的中央淋巴结转移 (CLM)。估计的 3 年和 5 年无复发生存率分别为 86.1% 和 84.4%。估计的 3 年和 5 年癌症特异性 OS 分别为 94.5% 和 92.2%。
结论
没有孤立的 CLM,以及我们系列中报告的癌症特异性 OS,支持常规使用 RC-D2 治疗 RCC。然而,D3 淋巴结清扫术可推荐用于特定患者,例如术前已知 CLM 或淋巴结转移靠近回结肠血管起源的患者。
































 京公网安备 11010802027423号
京公网安备 11010802027423号