Archives of Gynecology and Obstetrics ( IF 2.1 ) Pub Date : 2022-06-16 , DOI: 10.1007/s00404-022-06589-y Lin Ding 1 , Zhuofei Bi 1 , Jialing Wu 1 , Jianhong Zhu 2 , Yunfang Yu 2 , He-Rui Yao 3, 4 , Yi-Min Liu 1
|
Purpose
To evaluate the effects of adjuvant chemotherapy (CT) and radiotherapy (RT) on the survival of uterine carcinosarcoma (UCS) patients.
Methods
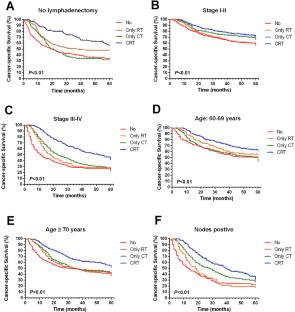
We analyzed 3207 patients with uterine carcinosarcoma without distant metastasis after surgery from 2004 to 2015 by utilizing data from the Surveillance, Epidemiology, and End Results database. Generally, cancer-specific survival (CSS) and overall survival (OS) outcomes were analyzed by Kaplan–Meier and Cox proportional hazards regression models. Further subgroup survival analysis was performed for those receiving RT and chemoradiotherapy (CRT).
Results
In general, both univariate and multivariate analyses showed that age, race, marital status, stage, lymph node metastasis, lymphadenectomy (LND), RT, and chemotherapy (CT) were associated with improved CSS and OS (P < 0.05). Further subgroup analysis showed that CRT exhibited a survival advantage over RT or CT alone in different groups. Various RT modalities, including brachytherapy (BT), external radiotherapy (EBRT), and EBRT + BT, were correlated with improved survival for patients aged 60–69 years with stage III–IV disease and lymph node metastasis. Patients with stage I–II disease aged > 70 years seemed to gain survival benefits from brachytherapy (BT) alone. BT with or without external radiotherapy was associated with improved survival for those who did not undergo lymphadenectomy.
Conclusion
For UCS without distant metastasis after surgery, CRT should be considered. Regarding RT, BT alone is efficient in improving survival, especially for patients with stage I–II disease aged > 70 years old. EBRT alone does not show results in survival improvement for patients who did not undergo LND and those with lymph node metastasis. However, considering the limitation of SEER database, further studies with more large sample size and strict study design are needed to confirm it.
中文翻译:
化疗和放疗在子宫癌肉瘤辅助治疗中的评价:基于人群的分析
目的
评估辅助化疗(CT)和放疗(RT)对子宫癌肉瘤(UCS)患者生存的影响。
方法
我们利用监测、流行病学和最终结果数据库中的数据分析了 2004 年至 2015 年 3207 例手术后无远处转移的子宫癌肉瘤患者。通常,通过 Kaplan–Meier 和 Cox 比例风险回归模型分析癌症特异性生存 (CSS) 和总生存 (OS) 结果。对接受放疗和放化疗 (CRT) 的患者进行了进一步的亚组生存分析。
结果
总的来说,单变量和多变量分析均显示年龄、种族、婚姻状况、分期、淋巴结转移、淋巴结清扫术 (LND)、放疗和化疗 (CT) 与 CSS 和 OS 改善相关( P < 0.05 ) 。进一步的亚组分析表明,在不同的组中,CRT 表现出优于单独 RT 或 CT 的生存优势。各种放疗方式,包括近距离放射治疗 (BT)、外放疗 (EBRT) 和 EBRT + BT,与 60-69 岁患有 III-IV 期疾病和淋巴结转移的患者的生存改善相关。年龄 > 70 岁的 I-II 期疾病患者似乎仅从近距离放射治疗 (BT) 中获得了生存益处。BT 联合或不联合外部放疗与未接受淋巴结清扫术的患者的生存率提高相关。
结论
对于术后无远处转移的UCS,应考虑CRT。关于 RT,单独 BT 可有效提高生存率,尤其是对于年龄 > 70 岁的 I-II 期疾病患者。对于未接受 LND 和淋巴结转移的患者,单独的 EBRT 并未显示出改善生存的结果。但是,考虑到SEER数据库的局限性,还需要更大样本量和严格研究设计的进一步研究来证实。
































 京公网安备 11010802027423号
京公网安备 11010802027423号