背景
2010 年,我们描述了一种针对 Rho GTP 酶激活蛋白 26(ARHGAP26,也称为与粘着斑激酶相关的 GTP 酶调节剂 [GRAF] 或寡肾上腺素样的新型免疫球蛋白 G (IgG) 自身抗体(在指示病例后称为抗 Ca)蛋白 1 [OPHN1L])在自身免疫性小脑共济失调 (ACA) 中的作用。后来,ARHGAP26-IgG/anti-Ca 被报道用于边缘性脑炎/认知衰退或周围神经病变的患者。在一些报告的病例中,该综合征与癌症有关。ARHGAP10/GRAF2 在整个中枢神经系统中表达,与 ARHGAP26/GRAF 具有显着的序列同源性。ARHGAP10 基因的突变与认知和精神症状以及精神分裂症有关。
客观的
评估 ARHGAP26-IgG/anti-Ca 是否与 ARHGAP10 发生共同反应。
方法
通过基于重组细胞的测定以及同种型和 IgG 亚类分析对 ARHGAP10/GRAF2 自身抗体进行血清学检测。
结果
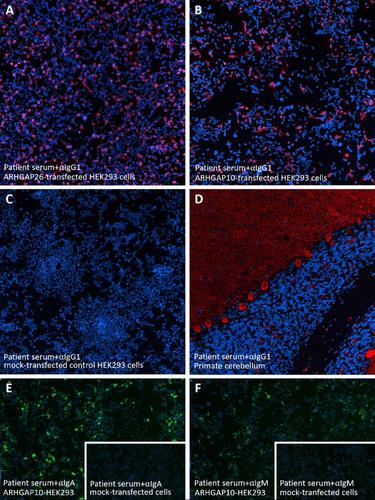
来自 9/12 (75%) ARHGAP26-IgG/抗 Ca 阳性患者的 26/31 血清样本 (84%) 和来自 4 名患者的 4/6 ARHGAP26-IgG/抗 Ca 阳性 CSF 样本也对 ARHGAP10 呈阳性-IgG。ARHGAP10-IgG(称为抗 Ca2)在长期(长达 109 个月)内仍可检测到,主要属于激活补体的 IgG1 亚类。中位 ARHGAP26-IgG/anti-Ca 和中位 ARHGAP10-IgG/anti-Ca2 血清滴度分别为 1:3200 和 1:1000,在某些样本中滴度异常高(ARHGAP26-IgG/anti-Ca: 高达 1: 1000,000;ARHGAP10-IgG:高达 1:32,000)。ARHGAP26/anti-Ca 血清滴度在所有样品中都超过了 ARHGAP10-IgG,但只有一个。一部分患者的 ARHGAP10-IgM 和 ARHGAP10-IgA 也呈阳性。CSF/血清比率和抗体指数计算表明 ARHGAP26-IgG/抗-Ca 和抗-ARHGAP10 的鞘内产生。在 101 个对照样本中,100 个 ARHGAP10-IgG 完全阴性;单个对照样品与 ARHGAP10 转染的细胞弱结合(1:10)。
结论
我们证明,很大一部分 ARHGAP26-IgG/抗 Ca 阳性自身免疫性脑炎患者与 ARHGAP10 有共同反应。需要进一步研究 ARHGAP10-IgG/抗 Ca2 血清阳性在自身免疫性脑炎患者中的临床和诊断意义。
 "点击查看英文标题和摘要"
"点击查看英文标题和摘要"
Rho GTPase-activating protein 10 (ARHGAP10/GRAF2) is a novel autoantibody target in patients with autoimmune encephalitis
Background
In 2010, we described a novel immunoglobulin G (IgG) autoantibody (termed anti-Ca after the index case) targeting Rho GTPase-activating protein 26 (ARHGAP26, also termed GTPase regulator associated with focal adhesion kinase [GRAF], or oligophrenin-like protein 1 [OPHN1L]) in autoimmune cerebellar ataxia (ACA). Later, ARHGAP26-IgG/anti-Ca was reported in patients with limbic encephalitis/cognitive decline or peripheral neuropathy. In several of the reported cases, the syndrome was associated with cancer. ARHGAP10/GRAF2, which is expressed throughout the central nervous system, shares significant sequence homology with ARHGAP26/GRAF. Mutations in the ARHGAP10 gene have been linked to cognitive and psychiatric symptoms and schizophrenia.
Objective
To assess whether ARHGAP26-IgG/anti-Ca co-reacts with ARHGAP10.
Methods
Serological testing for ARHGAP10/GRAF2 autoantibodies by recombinant cell-based assays and isotype and IgG subclass analyses.
Results
26/31 serum samples (84%) from 9/12 (75%) ARHGAP26-IgG/anti-Ca-positive patients and 4/6 ARHGAP26-IgG/anti-Ca-positive CSF samples from four patients were positive also for ARHGAP10-IgG. ARHGAP10-IgG (termed anti-Ca2) remained detectable in the long-term (up to 109 months) and belonged mainly to the complement-activating IgG1 subclass. Median ARHGAP26-IgG/anti-Ca and median ARHGAP10-IgG/anti-Ca2 serum titres were 1:3200 and 1:1000, respectively, with extraordinarily high titres in some samples (ARHGAP26-IgG/anti-Ca: up to 1:1000,000; ARHGAP10-IgG: up to 1:32,000). ARHGAP26/anti-Ca serum titres exceeded those of ARHGAP10-IgG in all samples but one. A subset of patients was positive also for ARHGAP10-IgM and ARHGAP10-IgA. CSF/serum ratios and antibody index calculation suggested intrathecal production of ARHGAP26-IgG/anti-Ca and anti-ARHGAP10. Of 101 control samples, 100 were completely negative for ARHGAP10-IgG; a single control sample bound weakly (1:10) to the ARHGAP10-transfected cells.
Conclusions
We demonstrate that a substantial proportion of patients with ARHGAP26-IgG/anti-Ca-positive autoimmune encephalitis co-react with ARHGAP10. Further studies on the clinical and diagnostic implications of ARHGAP10-IgG/anti-Ca2 seropositivity in patients with autoimmune encephalitis are warranted.
































 京公网安备 11010802027423号
京公网安备 11010802027423号