Surgical Endoscopy ( IF 2.4 ) Pub Date : 2022-05-13 , DOI: 10.1007/s00464-022-09306-7
Tanya Odisho 1 , Awni A Shahait 2 , Jared Sharza 3 , Abubaker A Ali 1, 2
|
Introduction
Minimally invasive or open Graham Patch repair remains the gold standard approach for management of perforated peptic ulcers (PPU). Herein, we report outcomes of laparoscopic technique and compare it with open approach at a community hospital.
Methods
Retrospective observational study conducted comparing laparoscopic modified Cellan-Jones repair (mCJR) versus the standard open repair of PPU. Patients aged 18–90 years during 2016–2021 were offered either a minimally invasive or open approach depending on surgeon laparoscopic capability, and were compared in terms of demographics, co-morbidities, intra-operative details, and short-term outcomes.
Results
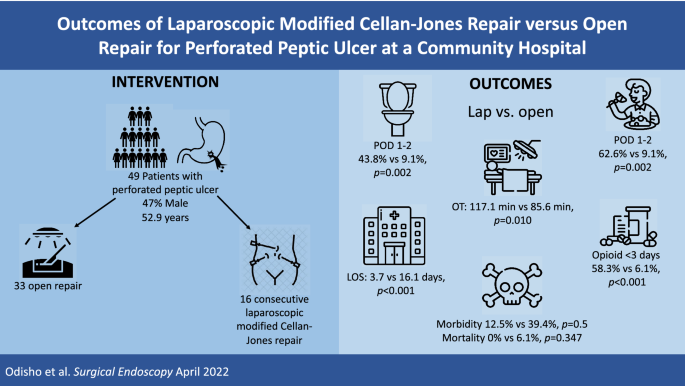
A total of 49 patients were included (46.9% males, mean age 52.9 years, mean BMI 25.0, ASA ≥ III 75.5%, 75.5% smokers, 26.5% current NSAIDs use, and 71.4% alcohol drinkers). Duodenum was the most common perforation site (57.1%), and majority of ulcers were 1–2 cm (72.9%). Laparoscopic approach was performed in 16 consecutive patients (32.7%) by a single surgeon, with no conversions. Preoperative characteristics were similar for both groups. Compared to open approach, laparoscopic group were taken to operation immediately (< 4 h) (87.5% vs. 15.2%, p < 0.001), had lower estimated blood loss (11.8 ml vs. 73.8 ml, p = 0.063), and longer operative time (117.1 min vs. 85.6 min, p = 0.010). Postoperatively, nasogastric tube was removed earlier in laparoscopic group (POD1-2, 87.5% vs. 24.2%, p = 0.001), with earlier resumption of diet (POD1-2, 62.6% vs. 9.1%, p = 0.002), less narcotic usage (< 3 days, 58.3% vs. 6.1%, p < 0.001), earlier return of bowel function (POD1-2, 43.8% vs. 9.1%, p = 0.003) and shorter length of stay (LOS) (3.7 days vs. 16.1 days, p < 0.001). Both in-house mortality and morbidity rates were lower in the laparoscopic group, but not statistically significant [(0% vs. 6.1%, p = 0.347) and (12.5% vs. 39.4%, p = 0.500), respectively].
Conclusion
Laparoscopic mCJR is a feasible method for repair of PPU, and it is associated with shorter LOS, and less narcotics usage in comparison to the open repair approach.
Graphical abstract
中文翻译:
社区医院消化性溃疡穿孔腹腔镜改良 Cellan-Jones 修复与开放修复的结果
介绍
微创或开放式 Graham Patch 修复仍然是治疗消化性溃疡穿孔 (PPU) 的金标准方法。在此,我们报告了腹腔镜技术的结果,并将其与社区医院的开腹手术进行了比较。
方法
比较腹腔镜改良 Cellan-Jones 修复术 (mCJR) 与 PPU 的标准开放修复术进行的回顾性观察研究。2016-2021 年间,根据外科医生的腹腔镜能力,为 18-90 岁的患者提供微创或开放手术,并在人口统计学、合并症、术中细节和短期结果方面进行了比较。
结果
总共包括 49 名患者(46.9% 为男性,平均年龄 52.9 岁,平均 BMI 25.0,ASA ≥ III 75.5%,75.5% 吸烟者,26.5% 目前使用非甾体抗炎药,71.4% 饮酒者)。十二指肠是最常见的穿孔部位 (57.1%),大多数溃疡为 1-2 厘米 (72.9%)。由一名外科医生对 16 名连续患者 (32.7%) 进行了腹腔镜手术,没有中转。两组的术前特征相似。与开腹手术相比,腹腔镜组立即进行手术(< 4 小时)(87.5% 对 15.2%,p < 0.001),估计失血量较低(11.8 ml 对 73.8 ml,p = 0.063),时间更长手术时间(117.1 分钟对 85.6 分钟,p = 0.010)。术后,腹腔镜组较早拔除鼻胃管(POD1-2,87.5% 对 24.2%,p = 0.001),较早恢复饮食(POD1-2,62.6% 对 9.1%,p = 0.002),较少麻醉剂使用(< 3 天,58.3% 对 6.1%,p < 0.001),肠功能更早恢复(POD1-2,43.8% 对 9.1%,p = 0.003)和更短的住院时间 (LOS) (3.7天对比 16.1 天,p < 0.001)。腹腔镜组的内部死亡率和发病率均较低,但无统计学意义[(分别为(0% 对 6.1%,p = 0.347)和(12.5% 对 39.4%,p = 0.500)]。
结论
腹腔镜 mCJR 是一种可行的 PPU 修复方法,与开放修复方法相比,它与更短的 LOS 和更少的麻醉剂使用有关。






























 京公网安备 11010802027423号
京公网安备 11010802027423号