目标
通过评估 PCT 后 Deauville 评分和 EBV DNA,确定新发转移性鼻咽癌 (mNPC) 患者是否会受益于接受根治性放疗 (DRT) 以及他们之前接受的姑息性化疗 (PCT)。
方法
共研究了 570 名接受 PCT 或 PCT+DRT 治疗的 mNPC 患者。EBV DNA 水平以及 PCT 后 Deauville 评分用于根据递归分区分析 (RPA) 对风险进行分层。
结果
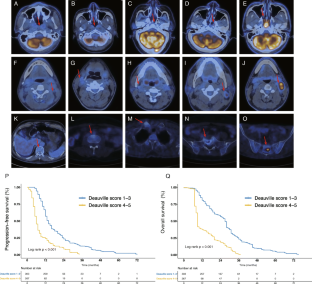
Deauville 评分为 1–3 和 4–5 的患者的生存率存在显着差异(2 年无进展生存率 (PFS):23.4% 对 8.5%,p < 0.001;2 年总生存率(OS ): 56.8% 对比 18.8%, p< 0.001)。RPA 按风险递增顺序产生了三个不同的组(所有 RPA I-II 的 Deauville 分数在 1–3 范围内):(1) RPA I:预处理浓度≤ 4000 拷贝/mL 且检测不到的 EBV DNA 水平PCT后;(2) RPA II:预处理浓度 > 4000 拷贝/mL 或预处理浓度 ≤ 4000 拷贝/mL 且在 PCT 后可检测到的 EBV DNA 水平;(3) RPA III:多维尔得分 4–5。虽然 RPA I 和 RPA II 患者在接受 PCT+DRT 治疗时的 PFS 率显着高于仅接受 PCT 治疗(RPA I:72.7% 对 13.4%,RPA II:37.8% 对 6.3%),但 RPA III 患者没有体验到这样的 PFS 益处(6.5% 对 9.7%)。
结论
PCT+DRT 可能会提高低危和中危 mNPC 患者的生存率,但不能提高高危患者的生存率。
关键点
 "点击查看英文标题和摘要"
"点击查看英文标题和摘要"
Determining the suitability of definitive radiation therapy in patients with metastatic nasopharyngeal carcinoma based on PET/CT: a large cohort study
Objectives
To determine patients with de novo metastatic nasopharyngeal carcinoma (mNPC) who would benefit from receiving definitive radiation therapy (DRT) along with their pre-existing palliative chemotherapy (PCT) by evaluating their post-PCT Deauville scores and EBV DNA.
Methods
A total of 570 mNPC patients, treated with PCT or PCT+DRT, were studied. EBV DNA levels, along with post-PCT Deauville scores, were used to stratify risk based on the recursive partitioning analysis (RPA).
Results
Significant differences were observed in the survival rates of patients with Deauville scores of 1–3 and 4–5 (2-year progression-free survival (PFS): 23.4% versus 8.5%, p < 0.001; 2-year overall survival (OS): 56.8% versus 18.8%, p < 0.001). RPA yielded three distinct groups in the increasing order of risk (Deauville scores of all RPA I-II were within the range of 1–3): (1) RPA I: EBV DNA levels at a pretreatment concentration ≤ 4000 copies/mL and undetectable post-PCT; (2) RPA II: EBV DNA levels either at a pretreatment concentration > 4000 copies/mL or at a pretreatment concentration ≤ 4000 copies/mL and detectable post-PCT; (3) RPA III: Deauville scores 4–5. While patients in RPA I and RPA II had significantly PFS rates when treated with PCT+DRT than when treated with PCT alone (RPA I: 72.7% versus 13.4%, RPA II: 37.8% versus 6.3%), those in RPA III did not experience such PFS benefits (6.5% versus 9.7%).
Conclusion
PCT+DRT might improve the survival rates in mNPC patients in the low- and mid-risk strata but not those of patients in the high-risk strata.
Key Points
































 京公网安备 11010802027423号
京公网安备 11010802027423号