Neurological Sciences ( IF 2.7 ) Pub Date : 2022-04-08 , DOI: 10.1007/s10072-022-06059-y Giulio Bonomo 1, 2 , Alberto Cusin 1 , Emanuele Rubiu 1, 2 , Guglielmo Iess 1, 2 , Paolo Ferroli 1 , Roberta Bonomo 3, 4 , Giorgio Battista Boncoraglio 3 , Mario Stanziano 5, 6
|
Background and purpose
Intradural disc herniation (IDH) can manifest with radicular or medullary syndrome. In about 15% of cases, IDH may be responsible, through a dural laceration, for a CSF leak, determining spontaneous intracranial hypotension (SIH) and CNS superficial siderosis (CNSss). This paper attempts to present an overview on IDH as the cause for both CSF leak, and subsequent SIH, and CNSss, and to describe a peculiar clinical and neuroradiological scenario related to this condition.
Methods
A search on the PUBMED database was performed. Although the investigation did not rigorously follow the criteria for a systematic review (we consider only articles about thoracic IDH), nonetheless, the best quality evidence was pursued. Furthermore, an illustrative case was presented.
Results
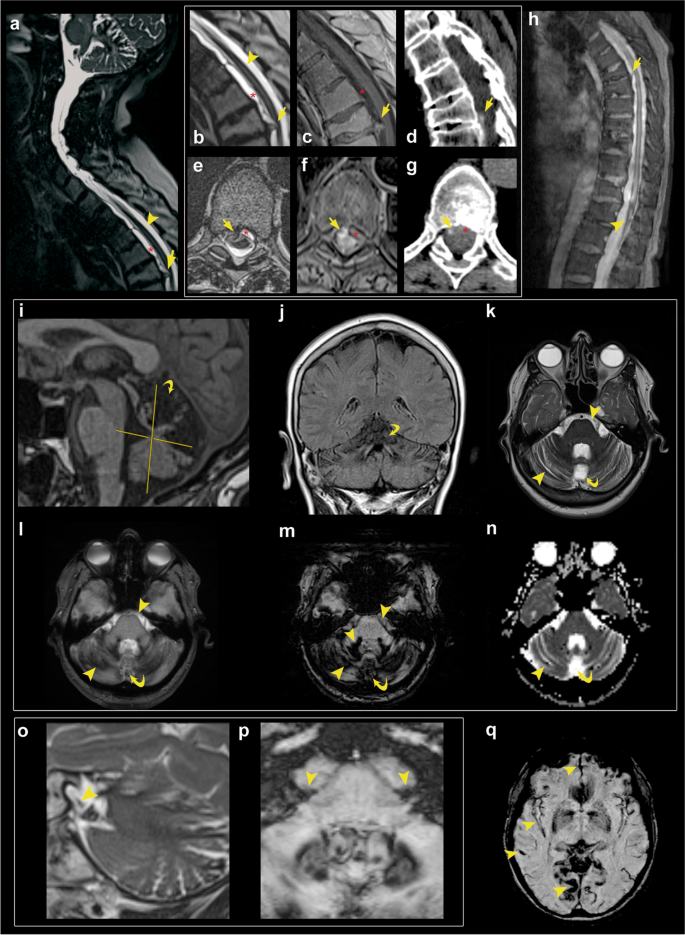
A 69-year-old woman was referred to our hospital for slowly progressive gait disturbances and hearing impairment. Brain imaging revealed diffuse bilateral supratentorial and infratentorial superficial siderosis, mostly of the cerebellum, the eighth cranial nerves, and the brainstem. Spinal imaging disclosed a posterior disc herniation determining a dural tear at D6-D7. Lumbar puncture revealed low opening pressure and hemorrhagic CSF with siderophages. A posterior transdural herniectomy and dural sealing determined a stabilization of hearing and a significant improvement in both gait and balance.
Conclusions
The diagnostic workup of CNSss with suspected CNS leak demands whole neuraxis imaging, especially in cases presenting SIH or myelopathic symptoms. This may avoid delays in detection of IDH and spinal dural leaks. The different forms of treatment available depend on the type and severity of the clinical picture.
中文翻译:
与脑脊液漏、颅内低血压和中枢神经系统表面铁质沉着症相关的硬膜内胸椎间盘突出症的诊断方法、治疗策略和手术指征
背景和目的
硬膜内椎间盘突出症 (IDH) 可表现为神经根或髓质综合征。在大约 15% 的病例中,IDH 可能通过硬脑膜撕裂导致脑脊液漏,确定自发性颅内低血压 (SIH) 和中枢神经系统表面铁质沉着症 (CNSss)。本文试图概述 IDH 作为 CSF 泄漏、随后的 SIH 和 CNSs 的原因,并描述与这种情况相关的特殊临床和神经放射学情况。
方法
对 PUBMED 数据库进行了搜索。尽管该调查并未严格遵循系统评价的标准(我们仅考虑有关胸部 IDH 的文章),但仍寻求质量最好的证据。此外,还介绍了一个说明性案例。
结果
一名 69 岁女性因缓慢进展的步态障碍和听力障碍被转诊到我院。脑成像显示弥漫性双侧幕上和幕下浅表铁质沉着症,主要位于小脑、第八对脑神经和脑干。脊柱成像显示后椎间盘突出,确定了 D6-D7 的硬脑膜撕裂。腰椎穿刺显示低开口压力和含铁噬菌体的出血性脑脊液。后部经硬膜疝切除术和硬脑膜封闭确定了听力的稳定以及步态和平衡的显着改善。
结论
疑似 CNS 渗漏的 CNSs 的诊断检查需要全神经轴成像,特别是在出现 SIH 或脊髓病症状的情况下。这可以避免延迟检测 IDH 和硬脊膜渗漏。可用的不同治疗形式取决于临床表现的类型和严重程度。






























 京公网安备 11010802027423号
京公网安备 11010802027423号