Abdominal Radiology ( IF 2.3 ) Pub Date : 2022-02-14 , DOI: 10.1007/s00261-022-03443-2
Samuel J Withey 1 , Dimitra Christodoulou 1 , Davide Prezzi 1 , Giles Rottenberg 1 , Cherry Sit 1, 2 , Fahim Ul-Hassan 2 , Paul Carroll 3 , Anand Velusamy 3 , Louise Izatt 4 , Rajesh Nair 5 , Audrey E T Jacques 1
|
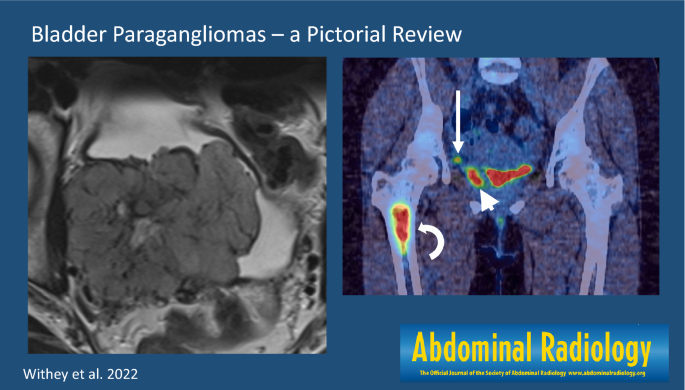
Bladder paragangliomas (bPGL) are rare neuroendocrine tumors arising from the sympathetic paraganglia present in the bladder wall. Bladder PGLs are typically submucosal or intramural but when subserosal may not be readily visible at cystoscopy. The average size at presentation is 3.9 cm (range 1.0–9.1 cm). When small, bPGL are usually spherical, well-marginated and homogeneous. Larger bPGL are typically more complex with peri- and intra-tumoral neovascularity and central necrosis. On ultrasound, increased color Doppler signal is typical. The increased soft tissue resolution of MRI enables localization of bPGL within the bladder wall more accurately than CT. Restricted diffusion and avid contrast enhancement help differentiate small bPGLs from leiomyomas, which have similar appearances on ultrasound and CT. Nuclear medicine techniques identify bPGLs and their metastases with high specificity, 68Ga-DOTATATE PET/CT having largely replaced 123I-mIBG SPECT/CT as the first line functional investigation. Imaging is essential to aid surgical planning, as endoscopic resection is often not possible or incomplete due to tumor location. For patients with advanced disease, 68Ga-DOTATATE PET/CT and 123I-mIBG SPECT/CT assess suitability for peptide receptor radionuclide therapy. Up to 63% of bPGL patients have a germline mutation, most commonly in the SDHB subunit gene, increasing their risk of developing pheochromocytomas and further paragangliomas; lifelong annual biochemical and periodic imaging screening from skull base to pelvis is therefore recommended.
Graphical abstract
中文翻译:
膀胱副神经节瘤:图片回顾
膀胱副神经节瘤 (bPGL) 是一种罕见的神经内分泌肿瘤,起源于膀胱壁中的交感神经副神经节。膀胱 PGL 通常位于黏膜下或壁内,但在膀胱镜检查中可能不容易看到浆膜下。展示时的平均尺寸为 3.9 厘米(范围 1.0–9.1 厘米)。当 bPGL 很小时,通常是球形的、边缘清晰且均匀的。较大的 bPGL 通常更复杂,伴有肿瘤周围和肿瘤内的新生血管和中央坏死。在超声上,增加的彩色多普勒信号是典型的。MRI 增加的软组织分辨率使 bPGL 在膀胱壁内的定位比 CT 更准确。限制性扩散和强烈的对比增强有助于区分小的 bPGL 与平滑肌瘤,后者在超声和 CT 上具有相似的外观。68 Ga-DOTATATE PET/CT 已在很大程度上取代123 I-mIBG SPECT/CT 作为一线功能检查。成像对于辅助手术计划至关重要,因为由于肿瘤位置,内窥镜切除通常是不可能的或不完整的。对于晚期疾病患者,68 Ga-DOTATATE PET/CT 和123 I-mIBG SPECT/CT 评估肽受体放射性核素治疗的适用性。高达 63% 的 bPGL 患者有种系突变,最常见的是 SDHB 亚基基因,这增加了他们患嗜铬细胞瘤和进一步副神经节瘤的风险;因此,建议进行从颅底到骨盆的终生年度生化和定期成像筛查。
































 京公网安备 11010802027423号
京公网安备 11010802027423号