背景
Kommerell 憩室 (KD) 是一种扩张的近端异常右或左锁骨下动脉,与右或左主动脉弓 (RAA-ARSA 或 LAA-ALSA) 相关。尽管病例系列表明 KD 可能导致血管并发症,但其风险、整个生命周期的扩张模式以及弓侧之间的差异尚不清楚。
方法
这项研究是一项单中心回顾性研究,对所有年龄的 KD 患者进行横断面成像。KD 的最大短轴直径 (KDmax),绝对值并与降主动脉直径 (DAo) 相关,与年龄相关。在拱侧之间进行了比较。描述了患有血管并发症的患者。
结果
共纳入 104 名 KD 患者:68 名(65%)患有 RAA-ALSA,36 名(35%)患有 LAA-ARSA,43 名(41%)无症状。虽然 KDmax 与年龄相关(RAA-ALSA r = 0.84;[ P < .0001];LAA-ARSA r = 0.51 [ P = .001]),但与 DAo 相关的 KDmax 与年龄无关(RAA-ALSA r = 0.14 [ P = .27];LAA-ARSA r = -0.22 [ P = .21])。RAA-ALSA 患者的 KDmax 与 DAO 相关(1.02 ± 0.20 mm/mm vs 0.89 ± 0.18 mm/mm;P = .002)和更多症状(75% vs 28%;P < .0001),并且他们是更年轻(中位数,9.5 岁 vs 61.7 岁;P< .0001)。6 名患者(58 至 80 岁)有血管并发症,所有 6 名患者都有 LAA-ARSA 和获得性动脉瘤的危险因素。
结论
在老年患者中,与 DAO 相关的 KDmax 并不大,因此反对单独的 KD 随着年龄的增长。RAA-ALSA 和 LAA-ARSA 的憩室表现出不同的表型,这一发现表明不同的疾病过程和可能不同的风险。血管并发症的发生率低于以前的报告,这些并发症仅发生在有 LAA-ARSA 和动脉瘤危险因素的患者中。这一发现表明,对无症状 KD 进行保守治疗通常是合理的,尤其是在 RAA-ALSA 患者中。
 "点击查看英文标题和摘要"
"点击查看英文标题和摘要"
Kommerell Diverticulum: Distinctions Between Arch Side and Evaluation of Morphology, Size, And Risk
Background
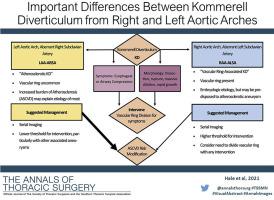
Kommerell diverticulum (KD) is a dilated proximal aberrant right or left subclavian artery associated with either right or left aortic arches (RAA-ARSA or LAA-ALSA). Although case series suggest that KD may be a liability for vascular complications, the risk, pattern of dilation throughout the life span, and differences between arch sides are not known.
Methods
This study was a single-center retrospective review of patients of all ages with KD on cross-sectional imaging. Maximal short-axis diameter of KD (KDmax), absolute and indexed to descending aortic diameter (DAo), was correlated with age. Comparisons were made between arch sides. Patients with vascular complications were described.
Results
A total of 104 patients with KD were included: 68 (65%) with RAA-ALSA, 36 (35%) with LAA-ARSA, 43 (41%) asymptomatic. Although KDmax was correlated with age (RAA-ALSA r = 0.84; [P< .0001]; LAA-ARSA r = 0.51 [P = .001]), KDmax indexed to DAo was not (RAA-ALSA r = 0.14 [P = .27]; LAA-ARSA r = −0.22 [P = .21]). Patients with RAA-ALSA had larger KDmax indexed to DAo (1.02 ± 0.20 mm/mm vs 0.89 ± 0.18 mm/mm; P = .002) and more symptoms (75% vs 28%; P < .0001), and they were younger (median, 9.5 years vs 61.7 years; P < .0001). Six patients (58 to 80 years of age) had vascular complications, and all 6 had LAA-ARSA and risk factors for acquired aneurysms.
Conclusions
In older patients, KDmax indexed to DAo was not larger, thus arguing against isolated KD dilation with age. Diverticula from RAA-ALSA and LAA-ARSA demonstrated different phenotypes, a finding suggesting different disease processes and likely different risk. The incidence of vascular complications was lower than in previous reports, and these complications occurred exclusively in patients with LAA-ARSA and aneurysm risk factors. This finding suggests that conservative management of asymptomatic KD is often reasonable, especially in patients with RAA-ALSA.





























 京公网安备 11010802027423号
京公网安备 11010802027423号