心血管疾病是全世界死亡的首要原因。在不同的心脏功能障碍中,钙化导致的心脏瓣膜衰竭仍然是一个具有挑战性的问题。虽然早期钙化的药物依赖性治疗可以减缓其进展,但晚期钙化不可避免地需要心脏瓣膜置换术。目前,心脏瓣膜置换主要有机械心脏瓣膜和生物心脏瓣膜两种。尽管这两种类型的瓣膜在恢复心脏功能方面具有显着的优势,但从长远来看,它们都存在严重的缺陷。一方面,机械性血流动力学表现出非生理性血流动力学,需要长期抗凝治疗。另一方面,生物的则由于钙化而表现出狭窄和/或反流。如今,新的有前途的心脏瓣膜替代品已经出现,称为脱细胞组织工程心脏瓣膜(dTEHV)。不同类型的脱细胞组织因其优越的生物力学、生物相容性和仿生材料成分而在生物假体和组织工程瓣膜中得到了广泛的测试。这些优点使得细胞能够成功附着、生长和发挥功能,最终形成体内活的再生瓣膜组织。然而,还没有全面的研究涵盖 dTEHV 支架在钙化问题效率方面的性能。在这篇综述文章中,我们试图回答脱细胞心脏瓣膜是否钙化的问题。此外,哪些因素使它们钙化,哪些因素降低和/或阻止它们的钙化。 此外,该综述讨论了与天然心脏瓣膜和生物假体心脏瓣膜的钙化相比,dTEHV 钙化的可能机制。为此,我们对所有已发表的脱细胞心脏瓣膜工作进行了回顾性研究。本次综述仅包括动物和临床研究。根据脱细胞化对钙化的影响,这些动物和临床研究进一步分为 4 类。由于心脏瓣膜钙化的复杂性,其他体外和计算机研究未包括在内。最后,我们比较了不同的结果并总结了脱细胞心脏瓣膜是否钙化的所有可靠发现。根据我们的审查,选择合适的心脏瓣膜组织来源(无免疫激发残留物)、脱细胞技术(脱细胞组织无受损暴露残留物、无死细胞残留、无脱细胞剂残留)和植入技术(避免即使没有体外细胞接种或额外的支架处理,也可以提供完美的抗钙化潜力。
 "点击查看英文标题和摘要"
"点击查看英文标题和摘要"
Decellularized tissue-engineered heart valves calcification: what do animal and clinical studies tell us?
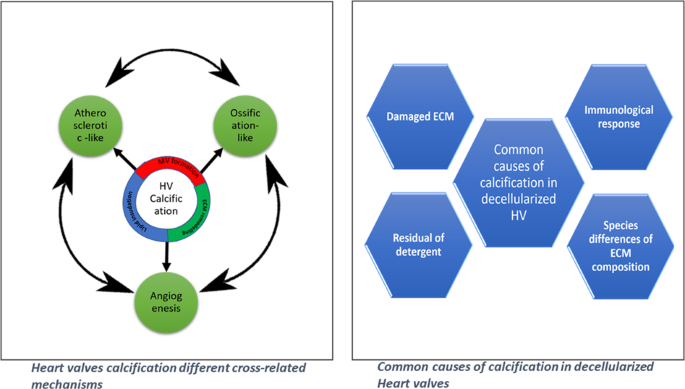
Cardiovascular diseases are the first cause of death worldwide. Among different heart malfunctions, heart valve failure due to calcification is still a challenging problem. While drug-dependent treatment for the early stage calcification could slow down its progression, heart valve replacement is inevitable in the late stages. Currently, heart valve replacements involve mainly two types of substitutes: mechanical and biological heart valves. Despite their significant advantages in restoring the cardiac function, both types of valves suffered from serious drawbacks in the long term. On the one hand, the mechanical one showed non-physiological hemodynamics and the need for the chronic anticoagulation therapy. On the other hand, the biological one showed stenosis and/or regurgitation due to calcification. Nowadays, new promising heart valve substitutes have emerged, known as decellularized tissue-engineered heart valves (dTEHV). Decellularized tissues of different types have been widely tested in bioprosthetic and tissue-engineered valves because of their superior biomechanics, biocompatibility, and biomimetic material composition. Such advantages allow successful cell attachment, growth and function leading finally to a living regenerative valvular tissue in vivo. Yet, there are no comprehensive studies that are covering the performance of dTEHV scaffolds in terms of their efficiency for the calcification problem. In this review article, we sought to answer the question of whether decellularized heart valves calcify or not. Also, which factors make them calcify and which ones lower and/or prevent their calcification. In addition, the review discussed the possible mechanisms for dTEHV calcification in comparison to the calcification in the native and bioprosthetic heart valves. For this purpose, we did a retrospective study for all the published work of decellularized heart valves. Only animal and clinical studies were included in this review. Those animal and clinical studies were further subcategorized into 4 categories for each depending on the effect of decellularization on calcification. Due to the complex nature of calcification in heart valves, other in vitro and in silico studies were not included. Finally, we compared the different results and summed up all the solid findings of whether decellularized heart valves calcify or not. Based on our review, the selection of the proper heart valve tissue sources (no immunological provoking residues), decellularization technique (no damaged exposed residues of the decellularized tissues, no remnants of dead cells, no remnants of decellularizing agents) and implantation techniques (avoiding suturing during the surgical implantation) could provide a perfect anticalcification potential even without in vitro cell seeding or additional scaffold treatment.






























 京公网安备 11010802027423号
京公网安备 11010802027423号