Journal of Pediatric Surgery ( IF 2.4 ) Pub Date : 2020-11-12 , DOI: 10.1016/j.jpedsurg.2020.11.009 Marion Durand 1 , Layla Musleh 2 , Fabrizio Vatta 3 , Giorgia Orofino 4 , Stefania Querciagrossa 4 , Myriam Jugie 5 , Olivier Bustarret 5 , Christophe Delacourt 6 , Sabine Sarnacki 7 , Thomas Blanc 7 , Naziha Khen-Dunlop 7
|
Background/Purpose
Lobectomy is required in children affected by non-responsive, symptomatic, localized bronchiectasis, but inflammation makes thoracoscopy challenging. We present the first published series of robotic-assisted pulmonary lobectomy in children with bronchiectasis.
Methods
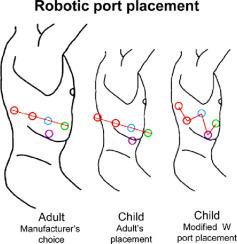
Retrospective analysis of all consecutive patients who underwent pulmonary lobectomy for severe localized bronchiectasis (2014–2019) via thoracoscopic versus robotic lobectomy. Four 5 mm ports were used for thoracoscopy; a four-arm approach was used for robotic surgery (Da Vinci Surgical Xi System, Intuitive Surgical, California).
Results
Eighteen children were operated (robotic resection, n = 7; thoracoscopy, n = 11) with infected congenital pulmonary malformation, primary ciliary dyskinesia, and post-viral infection. There were no conversions to open surgery with robotic surgery, but five with thoracoscopy. Total operative time was significantly longer with robotic versus thoracoscopic surgery (mean 247 ± 50 versus 152 ± 57 min, p = 0.008). There were no significant differences in perioperative complications, length of thoracic drainage, or total length of stay (mean 7 ± 2 versus 8 ± 3 days, respectively). No blood transfusions were required. Two thoracoscopic patients had a type-3 postoperative complication.
Conclusions
Pediatric robotic lung lobectomy is feasible and safe, with excellent visualization and bi-manual hand-wrist dissection – useful properties in difficult cases of infectious pathologies. However, instrumentation dimensions limit use in smaller thoraxes.
中文翻译:
重度支气管扩张儿童机器人肺叶切除术:一项有价值的新技术
背景/目的
受无反应、有症状、局部支气管扩张影响的儿童需要进行肺叶切除术,但炎症使胸腔镜检查具有挑战性。我们展示了第一个已发表的针对支气管扩张症儿童的机器人辅助肺叶切除术系列。
方法
通过胸腔镜与机器人肺叶切除术对所有因严重局部支气管扩张(2014-2019)进行肺叶切除术的连续患者进行回顾性分析。四个 5 mm 端口用于胸腔镜检查;四臂方法用于机器人手术(Da Vinci Surgical Xi System,Intuitive Surgical,California)。
结果
18 名 患有先天性肺畸形感染、原发性纤毛运动障碍和病毒感染后的儿童接受了手术(机器人切除术,n = 7;胸腔镜检查,n = 11)。机器人手术没有转换为开放手术,但胸腔镜手术有 5 个转换。机器人与胸腔镜手术的总手术时间明显更长(平均 247 ± 50 与 152 ± 57 分钟,p = 0.008)。围手术期并发症、胸腔引流时间或总住院时间没有显着差异(分别为平均 7±2 天和 8±3 天)。不需要输血。两名胸腔镜患者出现 3 型术后并发症。
结论
小儿机器人肺叶切除术是可行且安全的,具有出色的可视化和双手手腕解剖 - 在感染性疾病的疑难病例中非常有用。然而,仪器尺寸限制在较小的胸部使用。





























 京公网安备 11010802027423号
京公网安备 11010802027423号