Gastrointestinal Endoscopy ( IF 6.7 ) Pub Date : 2020-03-30 , DOI: 10.1016/j.gie.2020.03.3846 Masayasu Horibe 1 , Eisuke Iwasaki 2 , Fateh Bazerbachi 3 , Tetsuji Kaneko 4 , Juntaro Matsuzaki 2 , Kazuhiro Minami 2 , Tatsuhiro Masaoka 2 , Naoki Hosoe 5 , Yuki Ogura 6 , Shin Namiki 6 , Yasuo Hosoda 7 , Haruhiko Ogata 5 , Andrew T Chan 8 , Takanori Kanai 2
|
Background and Aims
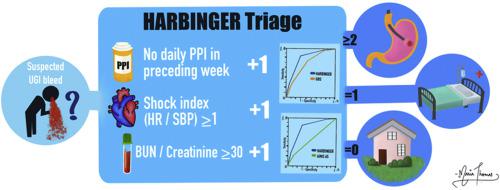
Although upper GI bleeding (UGIB) is a significant cause of inpatient admissions, no scoring method has proven to be accurate and simple as a standard for triage purposes. Therefore, we compared a previously described 3-variable score (1 point each for absence of daily proton pump inhibitor use in the week before the index presentation, shock index [heart rate/systolic blood pressure] ≥1, and blood urea nitrogen/creatinine ≥30 [urea/creatinine≥140]), the Horibe gAstRointestinal BleedING scoRe (HARBINGER), with the 8-variable Glasgow-Blatchford Score (GBS) and 5-variable AIMS65 to evaluate and validate the accuracy in predicting high-risk features that warrant admission and urgent endoscopy.
Methods
Consecutive patients presenting with suspected UGIB between 2012 and 2015 were prospectively enrolled in 3 acute care Japanese hospitals. On presentation to the emergency setting, an endoscopy was performed in a timely fashion. The primary outcome was the prediction of high-risk endoscopic stigmata.
Results
Of 1486 enrolled patients, 637 (43%) harbored high-risk endoscopic stigmata according to international consensus statements. The area under the receiver operating characteristic curve (AUC) for the HARBINGER was .76 (95% confidence interval [CI], .72-.79), which was significantly superior to both the GBS (AUC, .68; 95% CI, .64-.71; P < .001) and the AIMS65 (AUC, .54; 95% CI, .50-.58; P < .001). When the HARBINGER cutoff value was set at 1 to rule out patients who needed admission and urgent endoscopy, its sensitivity and specificity was 98.8% (95% CI, 97.9-99.6) and 15.5% (95% CI, 13.1-18.0), respectively.
Conclusions
The HARBINGER, a simple 3-variable score, provides a more accurate method for triage of patients with suspected UGIB than both the GBS and AIMS65.
中文翻译:
Horibe GI出血预测评分:可疑的上GI出血患者的分流决策的简单评分。
背景和目标
尽管上消化道出血(UGIB)是住院患者的重要原因,但没有一种评分方法被证明是准确且简单的分类标准。因此,我们比较了先前描述的3变量评分(在出现指数前一周没有使用质子泵抑制剂的情况,休克指数[心率/收缩压]≥1和血尿素氮/肌酐各1分) ≥30 [尿素/肌酐≥140]),Horibe胃肠道出血评分(HARBINGER),8变量格拉斯哥-布拉奇福德评分(GBS)和5变量AIMS65来评估和验证预测高危特征的准确性需要入院并进行紧急内镜检查。
方法
前瞻性在2012年至2015年之间连续出现UGIB的患者入选了3家日本急诊医院。在出现紧急情况时,及时进行了内镜检查。主要结果是预测高风险内镜下的柱头。
结果
根据国际共识声明,在1486名登记的患者中,有637名(43%)患有高风险的内窥镜柱头。HARBINGER的接收器工作特征曲线(AUC)下的面积为0.76(95%置信区间[CI] ,. 72-.79),显着优于两个GBS(AUC,0.68; 95%CI) ,.64-.71;P <.001)和AIMS65(AUC,.54; 95%CI,.50-.58;P <.001)。当将HARBINGER临界值设置为1以排除需要入院和急诊内镜检查的患者时,其敏感性和特异性分别为98.8%(95%CI,97.9-99.6)和15.5%(95%CI,13.1-18.0) 。
结论
HARBINGER是一个简单的3变量评分,它为可疑UGIB患者的分类提供了比GBS和AIMS65更准确的方法。
































 京公网安备 11010802027423号
京公网安备 11010802027423号